The Art of Charm is where self-motivated people, just like you, come to learn from the company’s coaches about to how to master human dynamics, relationships, and becoming your best self with the help of Johnny and AJ, the company’s founders. Johnny and AJ bring their 11 years of coaching experience from their famous Bootcamps, where they host clients in Los Angeles from all over the world and they share their stories, best practices and themselves on this weekly podcast. Not only does The A ...
…
continue reading
เนื้อหาจัดทำโดย The Physician Assistant Life | Smarty PANCE เนื้อหาพอดแคสต์ทั้งหมด รวมถึงตอน กราฟิก และคำอธิบายพอดแคสต์ได้รับการอัปโหลดและจัดหาให้โดยตรงจาก The Physician Assistant Life | Smarty PANCE หรือพันธมิตรแพลตฟอร์มพอดแคสต์ของพวกเขา หากคุณเชื่อว่ามีบุคคลอื่นใช้งานที่มีลิขสิทธิ์ของคุณโดยไม่ได้รับอนุญาต คุณสามารถปฏิบัติตามขั้นตอนที่แสดงไว้ที่นี่ https://th.player.fm/legal
ที่คล้ายกับ The Audio PANCE and PANRE Physician Assistant Board Review Podcast
A top podcast for healthcare leaders, with over one million downloads, Radio Advisory is your weekly download on how to untangle the industry's most pressing challenges to help leaders like you make the best business decisions for your organization. From unpacking major trends in care delivery—like site-of-care shifts and the rise of high-cost drugs—to demystifying stakeholder dynamics, to shining a spotlight on priorities that may get overlooked, we're here to help. Our hosts and seasoned r ...
…
continue reading
From the stuff your mother never told you, to the stuff your doctor never learned, On Health features taboo-busting conversations that demystify and de-stigmatize our bodies, all while bridging the gap between conventional medicine and wellness. Join Yale-trained MD & midwife Aviva Romm and her line-up of expert guests as they discuss everything from periods to menopause, sex to reproductive health politics, and motherhood to mental health. Each week, Dr. Romm will be exploring the science a ...
…
continue reading
How can business help solve society’s biggest challenges? Welcome to Series 3 of Take on Tomorrow, the award-winning podcast from PwC that examines the biggest problems facing society and the role business can—and should—play in solving them. This series, we’re welcoming broadcaster and journalist Femi Oke to the show. She joins podcaster and journalist Lizzie O’Leary, and together with industry innovators, tech trailblazers and visionary leaders from around the globe, they’ll explore timely ...
…
continue reading
From 4 x New York Times best-selling author Rachel Hollis comes the ultimate podcast for anyone looking for more joy and purpose in their lives. Featuring candid interviews with top performers in business, media, and lifestyle, as well as deep dives into topics like health and motivation, The Rachel Hollis Podcast has everything you need to level up your life!
…
continue reading
Join host and Harvard Business School Online Creative Director Chris Linnane as he sits down with HBS faculty to discuss business education in a way that’s both entertaining and insightful. The Parlor Room is your key to breaking down academic theory without sacrificing depth—all while gaining practical takeaways for navigating the business world.
…
continue reading
Join expert voices from Barbell Logic and others from the world of strength for resources to help you get strong for life. Get coaching options and more educational content at barbell-logic.com.
…
continue reading
Montgomery & Company (MoCo) is a weekly podcast and radio show hosted by two-time WNBA Champion and Co-Owner/Vice President of the Atlanta Dream, Renee Montgomery, in partnership with WABE Atlanta. Both insightful and compelling, MoCo features interviews with some of the world’s top athletes, entertainers, and innovators as well as roundtable discussions with Renee’s colleagues, friends, and family, about sports, culture and building generational wealth. Montgomery & Company: Sports, Cultu ...
…
continue reading
New episode every Wednesday! Join the Barbell Shrugged crew in conversations about fitness, training, and frequent interviews w/ CrossFit Games athletes!
…
continue reading
Welcome to Almost 30 - a supportive space to fuel your conscious evolution. Join us, LA-based best friends Krista Williams and Lindsey Simcik, for heart-centered, hilarious conversations and real, raw, impactful interviews with brilliant guests. We dive deep into topics like modern spirituality to health and wellness, aliens to entrepreneurship, social justice, and self development. With every episode, our mission is to empower you, expand what you think is possible and, make you laugh - a l ...
…
continue reading
Player FM - แอป Podcast
ออฟไลน์ด้วยแอป Player FM !
ออฟไลน์ด้วยแอป Player FM !

))
Podcast Episode 81: Internal Medicine EOR Cardiology Questions
Manage episode 256904377 series 97199
เนื้อหาจัดทำโดย The Physician Assistant Life | Smarty PANCE เนื้อหาพอดแคสต์ทั้งหมด รวมถึงตอน กราฟิก และคำอธิบายพอดแคสต์ได้รับการอัปโหลดและจัดหาให้โดยตรงจาก The Physician Assistant Life | Smarty PANCE หรือพันธมิตรแพลตฟอร์มพอดแคสต์ของพวกเขา หากคุณเชื่อว่ามีบุคคลอื่นใช้งานที่มีลิขสิทธิ์ของคุณโดยไม่ได้รับอนุญาต คุณสามารถปฏิบัติตามขั้นตอนที่แสดงไว้ที่นี่ https://th.player.fm/legal
 Welcome to episode 81 of the Audio PANCE and PANRE PA Board Review Podcast.
Welcome to episode 81 of the Audio PANCE and PANRE PA Board Review Podcast.
Join me as I cover ten internal medicine rotation EOR content blueprint questions from the Smarty PANCE physician assistant board and rotation review website.
Special from today’s episode:
- Check out the new Smarty PANCE Internal Medicine Rotation (EOR) Review Course
- Download your Free Trello Smarty PANCE PAEA Internal Medicine EOR Tracking Template
- Take the FREE Internal Medicine Rotation Cardiovascular Practice Exam
- View the interactive Smarty PANCE Internal Medicine Rotation (EOR) Topic List
Below you will find an interactive exam to complement the podcast.
The Audio PANCE/PANRE and EOR PA Board Review Podcast
I hope you enjoy this free audio component to the examination portion of this site. The full board review course includes over 2,000 interactive board review questions and is available to all members of the PANCE and PANRE Academy and Smarty PANCE.
- You can download and listen to past FREE episodes here, on iTunes, on Google Play Music or Stitcher Radio.
- You can listen to the latest episode, take an interactive quiz and download more resources below.
Listen Carefully Then Take The Practice Exam
If you can’t see the audio player click here to listen to the full episode.
Podcast Episode 81: Ten Internal Medicine EOR Cardiology Questions
The following questions are linked to PAEA Content Blueprint lessons from the Smarty PANCE and PANRE Board Review Website. If you are a member you will be able to log in and view this interactive video lesson.
1. 55-year-old woman is admitted to the hospital because she has shortness of breath and pain on both sides of her chest with deep breathing which has worsened over the past 5 days. In recent weeks, she has been feeling fatigued and has had low-grade fevers and night sweats, and was found to have a new cardiac murmur on examination. Her temperature is 38.1°C (100.6°F), pulse is 106/min, respirations are 26/min, and blood pressure is 136/88 mm Hg. She appears diaphoretic and is in mild respiratory distress. Cardiac auscultation reveals a faint systolic murmur heard over the lower left sternal border. Her neck veins are distended and abdominal examination shows hepatomegaly. Which of the following is the most likely cause of her clinical presentation?
A. Fat embolism
B. Infective endocarditis
C. Myocardial infarction
D. Rheumatic fever
E. Small cell lung cancer
Click here to see the answer
Answer: B, Infective endocarditis
Infective endocarditis (IE) is an infection of the endocardial surfaces of the heart, most commonly the heart valves. IE occurs when a microorganism begins to invade the heart valves causing an inflammatory reaction that damages the valve – sometimes leading to stenosis and sometimes leading to regurgitation. This patient developed a new cardiac murmur in recent weeks that is described as a faint systolic murmur heard over the lower left sternal border. This is most consistent with tricuspid regurgitation. She also has distended neck veins and hepatomegaly, both of which suggest right-sided heart failure which can result from tricuspid regurgitation. Small infectious emboli can break away from the primary lesion on the tricuspid valve and go into the pulmonary vasculature causing shortness of breath and pleuritic chest pain. Most cases of IE are caused by Staphylococcus aureus and Viridans streptococci, and diagnosis is confirmed by obtaining multiple blood cultures that show that there is continuous bacteremia.
- Fat embolism to the pulmonary circulation almost always occurs with major trauma, including surgical procedures like intramedullary nailing of long bones. Fat emboli can occlude the microvasculature, triggering a systemic inflammatory response. The woman did not have recent trauma, and a fat embolism would not explain her cardiac murmur.
- Clinical presentation of myocardial infarction most often includes substernal crushing chest pain, radiation of pain to the arms, left shoulder, back, neck, and jaw, as well as shortness of breath, anxiety, and fatigue. A myocardial infarction would not explain her developing a new cardiac murmur in recent weeks.
- Rheumatic fever is an autoimmune inflammatory process that develops as a sequela of streptococcal infection. Clinical manifestations include polyarthritis, carditis, erythema marginatum, chorea, and subcutaneous nodules. Rheumatic fever can cause some of the symptoms seen in this case, but the acute onset makes this option less likely.
- Although small cell lung cancer can present with pulmonary symptoms and low grade fevers, it wouldn’t easily explain her new cardiac murmur or the signs of right-sided heart failure.
Review PAEA EOR Blueprint Pearls With Links to Topic Lesson: Internal Medicine Rotation: Cardiovascular (PEARLS) ⇒ Endocarditis
2. A 54-year-old man comes to the emergency department following a four-day history of left-sided chest pain and shortness of breath. One week ago, he experienced upper respiratory symptoms along with myalgias and general fatigue. He has no known past medical history. He has not traveled outside the US. His temperature is 38.1°C (100.6°F), pulse is 104/min, respirations are 17/min, oxygen saturation is 94% on room air, and blood pressure is 100/72 mm Hg. Physical examination shows an ill-appearing man with bibasilar rales, jugular venous distention of 11 cm with no murmurs, rubs, or gallops, and 1+ bilateral pitting edema of the lower extremities. His labs are within normal limits and his blood cultures are negative. An echocardiogram shows an ejection fraction of 35%. Which of the following is the most likely cause of this patient’s condition?
A. Adenovirus
B. Coxsackie A virus
C. Staphylococcus aureus
D. Corynebacterium diphtheriae
Click here to see the answer
The answer is A. Adenovirus
Myocarditis in the United States is most commonly caused by a viral infection, typically adenovirus, coxsackie B, parvovirus B19, or others. It often presents with systemic symptoms such as fatigue and chest pain, but may cause sudden death.
- Though coxsackie B virus is one of the most common causal pathogens of acute myocarditis, Coxsackie A causes herpangina, aseptic meningitis, and hand, foot, and mouth disease.
- Staphylococcus aureus is a common cause of bacterial endocarditis, not myocarditis. Endocarditis is more likely to present with a new murmur and signs of distant emboli such as nail-bed hemorrhage and Janeway lesions.
- Corynebacterium diphtheriae is the causal agent of diphtheria, which may involve myocarditis. However, the patient would then most likely have other symptoms of the disease, including pseudomembranous pharyngitis, lymphadenopathy, or an arrhythmia.
Review PAEA EOR Blueprint Pearls With Links to Topic Lesson: Internal Medicine Rotation: Cardiovascular (PEARLS) ⇒ Myocarditis
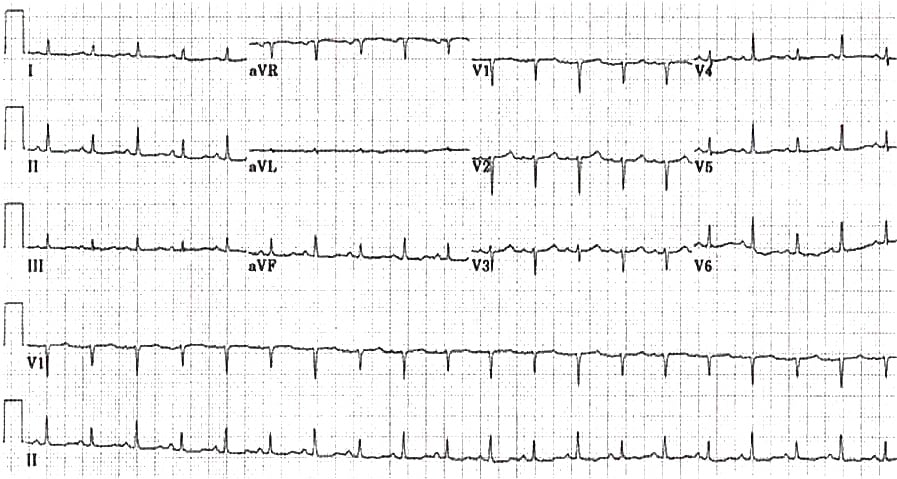
3. A 42-year-old woman comes to the emergency department because of chest pain, dyspnea, and lightheadedness. She recently recovered from a presumed viral upper respiratory infection and has a 10-year history of systemic lupus erythematosus. Physical examination shows a decrease in systolic blood pressure by 20 mm Hg during inspiration. An ECG is shown here. Which of the following is the most likely diagnosis?
A. Aortic dissection
B. Tricuspid regurgitation
C. Pericardial effusion
D. Aortic stenosis
E. Mitral stenosis
Click here to see the answer
The answer is C. Pericardial effusion
Pericardial effusions are associated with a variety of causes, including autoimmune disorders and infectious pericarditis. If pericardial effusion leads to cardiac tamponade, patients may have pulsus paradoxus, or a decrease in systolic blood pressure during inspiration of more than 10 mm Hg. Certain ECG findings are characteristic for pericardial effusion. In particular, electrical alternans (shown by arrows) is highly specific for pericardial effusion (usually in association with cardiac tamponade) but not particularly sensitive. This pattern, characterized by beat-to-beat changes in the QRS axis in the limb and precordial leads, is caused by swinging of the heart within the accumulated pericardial fluid. Other common findings on ECG include sinus tachycardia and low QRS voltage.
- Patients with aortic dissection classically present with a tearing or ripping pain in the chest or back and may have a significant variation in systolic blood pressure between arms (not across respirations).
- The severity of tricuspid regurgitation varies widely, ranging from asymptomatic disease to symptoms of right-sided heart failure (hepatosplenomegaly, ascites, peripheral edema).
- Patients with aortic stenosis, the most common cause of left ventricular outflow obstruction, typically present with exertional dizziness or angina. In end-stage disease, symptoms may progress to heart failure.
- Mitral stenosis obstructs the flow of blood from the left atrium to the left ventricle and typically manifests as exertional dyspnea and decreased exercise tolerance.
Review PAEA EOR Blueprint Pearls With Links to Topic Lesson: Internal Medicine Rotation: Cardiovascular (PEARLS) ⇒ Pericarditis
4. A 57-year-old man comes to the emergency department because of intermittent, severe leg pain in both his calves for 2 weeks. He has a history of untreated high blood pressure, diabetes, and high cholesterol. For the past 3 years, the pain started after walking three blocks and only going away upon resting. In the past 2 weeks, he has had the same pain at rest. His temperature is 36.5°C (97.7°F), pulse is 78/min, respirations are 17/min, and blood pressure is 160/89 mm Hg. Examination shows both calves are atrophied and there is a paucity of hair, but no swelling or discoloration. Additionally, his lower calves are cool to the touch and dusky in appearance. Doppler ultrasound shows perfusion to both feet, and blood pressures of 35/20 mm Hg in the posterior tibial artery are obtained bilaterally. Which of the following is most appropriate next step in management?
A. Immediate high-dose statin therapy
B. Immediately consult vascular surgery
C. Intravenous alteplase
D. Pain control and discharge; refer to vascular surgery as an outpatient
E. Rest, elevate, and compress the affected leg
Click here to see the answer
The answer is B. Immediately consult vascular surgery
Peripheral vascular disease with intermittent claudication and signs of decreased perfusion should be examined using Doppler ultrasound and the ankle-brachial index (ABI). An ABI of <0.41 is grounds for the immediate surgical consultation.
- Statin therapy has shown to be effective in treating intermittent claudication. However, this intervention is appropriate only when the patient is deemed to be stable, and the risk of limb ischemia has been addressed.
- Alteplase (tPa) has been used to treat intermittent claudication, but its use is outside the scope of the emergency room. Treatments initiated in the emergency department are unfractionated heparin, aspirin, pain control, and positioning of the leg to maintain perfusion.
- The patient has significant impairment of perfusion to his legs. Discharge and vascular surgery follow-up as an outpatient would be inappropriate and likely to result in morbidity or mortality.
- While this leg should be rested, compression and elevation are the opposite of what is needed. These therapies will further decrease the blood flow to the leg and put the patient at increased risk of complications.
Review PAEA EOR Blueprint Pearls With Links to Topic Lesson: Internal Medicine Rotation: Cardiovascular (PEARLS) ⇒ Peripheral vascular disease
5. A 6-year-old boy comes to the pediatric clinic because of 4 weeks of fatigue and shortness of breath. His medical history is notable for poor follow-up with yearly check-ups, but his mother notes that he has been fairly healthy for the duration of his life, except for a “bad sore throat that needed antibiotics” about 6 months ago. On examination, the boy appears fatigued, but is appropriately oriented and responsive, and is generally non-toxic appearing. He is afebrile. Cardiac examination is notable for a widely split S2, a quiet S1, and point of maximum impulse displaced to the left. Which of the following is the next best step in the management of this patient?
Elimination tool
A. Digoxin
B. Long-term penicillin
C. Short-term course of clindamycin
D. Reassurance & routine care
E. Intramuscular ceftriaxone
Click here to see the answer
The answer is B. Long-term penicillin
Rheumatic heart disease is caused by autoimmune cross-reactivity following a Streptococcal infection. Development of antibody-mediated mitral valve damage is common. Long-term penicillin is suitable for acute treatment and prophylaxis from complications.
- Digoxin is a purified cardiac glycoside that is typically used in the treatment of various heart conditions, such as atrial fibrillation, atrial flutter, and heart failure that cannot be controlled by other medication. It is not recommended for use in rheumatic fever.
- Clindamycin is an antibiotic used to treat middle ear infections, bone or joint infections, pelvic inflammatory disease, strep throat, pneumonia, and endocarditis. Clindamycin is typically used as endocarditis prophylaxis for patients that are already receiving penicillin for secondary rheumatic fever prophylaxis.
- This patient is suffering from rheumatic fever, which can lead to rheumatic heart disease. This can cause significant carditis which manifests as congestive heart failure.
- Ceftriaxone is an antibiotic used to treat numerous bacterial infections, such as pneumonia, ear infections, skin infections, urinary tract infection, and meningitis. It is not used in the treatment of rheumatic fever.
Review PAEA EOR Blueprint Pearls With Links to Topic Lesson: Internal Medicine Rotation: Cardiovascular (PEARLS) ⇒ Rheumatic heart disease
6. A 35-year-old woman, gravida 2, para 1, comes to the office because of her first prenatal visit at 12 weeks’ gestation. She has no current concerns, and her first child was born without complications. She has a history of long-standing untreated hypertension. Her temperature is 36.5°C (97.7°F), pulse is 78/min, respirations are 17/min, and blood pressure is 150/89 mm Hg. Which of the following medications would most likely be appropriate as initial treatment?
A. Atenolol
B. Hydrochlorothiazide
C. Labetalol
D. Lisinopril
E. Losartan
Click here to see the answer
The answer is C. Labetalol
Chronic hypertension in pregnancy can be treated with some medications and labetalol is recommended as a first-line therapy for treatment of hypertension during pregnancy. Angiotensin-converting enzymes (ACE) inhibitors and angiotensin II receptor blockers (ARBs) should be avoided.
- Atenolol is a β-blocker medication, which decreases blood pressure by decreasing heart rate and stroke volume. It is contraindicated in pregnancy because it has been associated with fetal growth restriction. β-blockers considered safe in pregnancy are metoprolol and labetalol.
- Hydrochlorothiazide is a thiazide diuretic which decreases blood pressure via volume depletion. Diuretics do not cause fetal malformations but are generally avoided in pregnancy, as they prevent the physiologic volume expansion seen in normal pregnancy. They may be used in states of volume-dependent hypertension, such as renal or cardiac disease.
- Lisinopril is an angiotensin-converting enzyme (ACE) inhibitor which decreases blood pressure through inhibition of the renin-angiotensin-aldosterone system. ACE inhibitors and the closely related angiotensin-receptor blockers are contraindicated in pregnancy because of the risk of birth defects including renal dysgenesis and oligohydramnios.
- Losartan is an angiotensin II receptor blocker (ARB) which decreases blood pressure through inhibition of the renin-angiotensin-aldosterone system. ARBs and the closely related angiotensin converting enzyme (ACE) inhibitors are contraindicated in pregnancy because of the risk of birth defects including renal dysgenesis and oligohydramnios.
Review PAEA EOR Blueprint Pearls With Links to Topic Lesson: Internal Medicine Rotation: Cardiovascular (PEARLS) ⇒ Hypertension
7. A 42-year-old man comes to the office for a routine check-up. Medical history includes diabetes mellitus and a long history of smoking. Family history includes coronary artery disease. Temperature is 36.5°C (97.7°F), pulse is 78/min, respirations are 17/min, and blood pressure is 160/89 mm Hg. A repeat blood pressure taken 2 days later shows 143/88 mm Hg. Which of the following is most likely the best initial therapy?
A. Enalapril
B. Furosemide
C. Hydrochlorothiazide
D. Metoprolol
E. Nifedipine
Click here to see the answer
Answer: A. Enalapril
Hypertension in the setting of diabetes should be treated, with a goal systolic blood pressure of <130 mm Hg. The best first choice of medication is an angiotensin-converting enzyme inhibitor (ACEi).
Incorrect Answers:
- Furosemide is a loop diuretic that can be used to treat hypertension but it is not a first line agent. Unlike ACE inhibitors, loop diuretics have no renoprotective qualities and therefore are a worse initial choice in a hypertensive diabetic patient.
- Hydrochlorothiazide is a thiazide diuretic and a first-line agent for the treatment of hypertension in non-diabetic patients. It is relatively contraindicated in diabetes because it has the potential adverse effect of hyperglycemia. It may also precipitate attacks of gout by increasing uric acid concentrations.
- Metoprolol is a β-blocker that is used for the treatment of hypertension but is not a first line treatment. Also, β-blocker are contraindicated in asthma, as well as in diabetic patients due to its potential to mask signs of low blood sugar.
- Nifedipine is a calcium channel blocker that is used in the treatment of hypertension but it is not a first line therapy. It has no renoprotective effects, and commonly causes peripheral edema as an unwanted adverse effect.
Review PAEA EOR Blueprint Pearls With Links to Topic Lesson: Internal Medicine Rotation: Cardiovascular (PEARLS) ⇒ Hypertension
8. A 45-year-old obese Caucasian gentleman arrives at your clinic for a routine check-up after having some blood work done during a workplace health screening. He is found to have an LDL cholesterol level of 550 mg/dL. He states that his father and brother had high cholesterol and both died at a young age from a heart attack. He has a follow-up appointment with his cardiologist because of some occasional chest pain and abnormalities seen on his EKG. Additionally, you notice that he has well-demarcated yellow deposits around his eyes. He is started on high dose statin and his LDL at 12 weeks is 350 mg/dL. What is the next best step in this patient’s management?
A. Continue high dose statin, the patient’s LDL is at goal
B. Add niacin 100 mg three times daily
C. Add ezetimibe (Zetia) 10 mg daily
D. Add a PCSK9 inhibitor
E. Refer to a lipid specialist
Click here to see the answer
The answer is C: add ezetimibe 10 mg
If LDL-C is not at goal after 6-12 weeks the next best step for the treatment of familial hypercholesterolemia is to add ezetimibe 10 mg daily and check again in 6-12 weeks. If at that time the patient’s LDL is still not at goal (ideally < 150) refer to lipid specialist to consider adding a PCSK9 inhibitor.
Pearls
- Familial hypercholesterolemia (FH) is the most common autosomal dominant genetic disease. The clinical syndrome (phenotype) is characterized by extremely elevated levels of low-density lipoprotein cholesterol (LDL-C) and a propensity to early-onset atherosclerotic cardiovascular disease. In general, homozygotes manifest the disease at a much earlier age than heterozygotes and the disease is more severe.
- Homozygous FH patients are rare and have an estimated prevalence of approximately 1:300,000 to 1:400,000
- Heterozygous FH is estimated to occur in 1 in 200 to 250 individuals in the United States.
- It is estimated that about 7 percent of American adults have an untreated lipoprotein cholesterol ≥190 mg/dL but only 1.7 percent carry an FH mutation
- Patients with undiagnosed homozygous familial hypercholesterolemia (FH) develop severe, premature, atherosclerotic cardiovascular disease and die before age 20 in many cases.
- In patients with a negative or unknown family history, an untreated LDL-C level of ≥190 mg/dL (4.9 mmol/L) suggests FH. This value is greater than the 90th percentile for age and sex.
Diagnosis
- The diagnosis of heterozygous familial hypercholesterolemia (FH) is made with genetic testing or clinical criteria. A causative mutation in the LDLR, APOB, or PCSK9 gene(s) secures this diagnosis
- When genetic testing is not available or not felt to be necessary, you can use the Dutch Lipid Clinic Network criteria, which assigns points based on low-density lipoprotein cholesterol (LDL-C) levels, personal history of early atherosclerotic cardiovascular disease (ASCVD), family history of early ASCVD, or high cholesterol in a first-degree relative, and personal and physical examination finding
Treatment
- Patients with homozygous familial hypercholesterolemia (FH) – intensive LDL-C lowering, which targets a minimal value of <150 mg/dL (3.9 mmol/L)
- In addition to a high-dose statin (atorvastatin 80 mg daily or rosuvastatin 40 mg daily), most homozygous patients will require additional therapies such as ezetimibe, a PCSK9 inhibitor, or potentially LDL-C apheresis
Review PAEA EOR Blueprint Pearls With Links to Topic Lesson: Internal Medicine Rotation: Cardiovascular (PEARLS) ⇒ Hyperlipidemia
9. A 65-year-old man comes to the emergency department because of progressive dyspnea, coughing, and orthopnea. The patient says that over the past 2 months he has been feeling fatigued with ordinary physical activity. His medical history is relevant for dyslipidemia, type II diabetes mellitus, and a posterior myocardial infarction 4 months ago. Auscultatory findings reveal a pansystolic murmur over the mitral area. His temperature is 37.5°C (99.5°F), pulse is 90/min, respirations are 17/min, blood pressure is 120/90 mm Hg, and pulse oximetry on room air shows an oxygen saturation of 95%. This patient most likely has which of the following conditions?
A. Aortic stenosis
B. Aortic valve regurgitation
C. Mitral valve regurgitation
D. Mitral valve stenosis
E. Pulmonary stenosis
Click here to see the answer
The answer is C. Mitral valve regurgitation
Mitral valve regurgitation is defined as an incompetent closure of the mitral valve. Classically patients will present with a pansystolic heart murmur over the mitral area. Posterior myocardial infarction is the second most common cause of mitral valve regurgitation. Mitral valve regurgitation is characterized by an incompetent closure of the mitral valve. This condition causes retrograde blood flow into the left atrium during systole. The most common cause of mitral regurgitation is mitral valve prolapse, followed by a dysfunction of the posteromedial papillary muscle due to posterior myocardial infarction. Other causes may include, endocarditis or stretching of the mitral valve ring.
- Aortic stenosis is the reduction of the valvular orifice (<2 cm) with left ventricular outflow obstruction. Patients with aortic stenosis present with chest pain, syncopal episodes, and dyspnea. Here, the patient has progressive dyspnea (NYHA II), and a pansystolic murmur (mitral area), which relates to mitral valve regurgitation
- Aortic valve regurgitation (AOR) is described as an inefficient closure of the aortic valve leading to a retrograde blood flow into the left ventricle during diastole. Patients will present with a wide pulse pressure (Corrigan hammer pulse) or an Austin-Flint murmur (severe), none of which are present in this case.
- Mitral valve stenosis (MVS) is the reduction of the mitral valve orifice (<2.5cm). The left atrium becomes dilated and hypertrophied because of increased work of the left atrium. Patients with MVS present with dyspnea, rust-colored sputum, atrial fibrillation, and a diastolic heart murmur (diastolic rumble and opening snap).
- Pulmonary stenosis is an uncommon valvular lesion. It is commonly associated with congenital heart disease and carcinoid heart disease. Patients present a systolic ejection murmur in the left second intercostal space.
Review PAEA EOR Blueprint Pearls With Links to Topic Lesson: Internal Medicine Rotation: Cardiovascular (PEARLS) ⇒ Valvular heart disease
10. A 43-year-old man with a history of rheumatic fever comes to the primary care clinic for a check up. Cardiac examination reveals a late systolic crescendo murmur with midsystolic click best heard over the apex and loudest just before S2. Which of the following maneuvers will cause an earlier onset of the click/murmur?
A. Inspiration
B. Rapid squatting
C. Standing
D. Hand grip
E. Left lateral cubital position
Click here to see the answer
The answer is C. Standing
The ‘click’ of mitral valve prolapse, caused by the tightening of the chordae tendinae, moves closer to S2 with increased preload. Increased preload causes the left ventricle to stretch, as a result, the chordae tendinae are stretched as well. This makes it harder for the mitral valve to prolapse until the ventricles shrink enough to allow the chordae tendinae to let the mitral valve prolapse. Since there is more blood in the ventricles, it takes them longer to pump it out and shrink to a point at which MVP can occur, hence it occurs later in systole. Thus, the click will get closer to S2 with increased preload. Hand grip, rapid squatting, and inspiration all increase preload. Standing decreases preload and will cause an earlier onset of the click.
- The click of mitral valve prolapse is heard closer to S2 in the event of increased preload. Preload is increased by hand grip, squatting and inspiration.
- Placing the patient in the left lateral cubitus position will not affect preload and will have no effect on the timing of the click in mitral valve prolapse.
Review PAEA EOR Blueprint Pearls With Links to Topic Lesson: Internal Medicine Rotation: Cardiovascular (PEARLS) ⇒ Heart murmurs
Looking for all the podcast episodes?
This FREE podcast series is limited to every other episode, you can download and enjoy the complete audio series by becoming a Smarty PANCE member.
I will be releasing new episodes every few weeks. Smarty PANCE is now discounted, so sign up now before it’s too late!
Resources and Links From The Show
- Check out the new Smarty PANCE Internal Medicine Rotation (EOR) Review Course
- Download your Free Trello Smarty PANCE PAEA Internal Medicine EOR Tracking Template
- Take the FREE Internal Medicine Rotation Cardiovascular Practice Exam
- View the interactive Smarty PANCE Internal Medicine Rotation (EOR) Topic List
- Follow Smarty PANCE and The Daily PANCE Blueprint on Instagram
- Follow SMarty PANCE and The Daily PANCE Blueprint on Facebook
- My list of recommended PANCE and PANRE review books
- Interactive PANCE and PANRE NCCPA Exam Content Blueprints
- Sign up for the FREE Daily PANCE and PANRE email series
- Join the Smarty PANCE NCCPA Content Blueprint Website
- Get your free Trello PANCE study schedule
- Get 20% of any Picmonic membership by using this link
- Use Code “PALIFE” and get 10% OFF THE RUTGERS PANCE AND PANRE REVIEW COURSE
This Podcast is also available on iOS and Android
- iTunes: The Audio PANCE and PANRE Podcast iTunes
- Stitcher Radio: The Audio PANCE and PANRE Podcast Stitcher
- Google Play: The Audio PANCE and PANRE Podcast Google Play
![]()
Download The Content Blueprint Checklist
Follow this link to download your FREE copy of the PANCE Content Blueprint Checklist
Print it up and start crossing out the topics you understand, marking the ones you don’t, and making notes of key terms you should remember. The PDF version is interactive and linked directly to the individual lessons on Smarty PANCE.
Download for PANCE Download for PANRE
The post Podcast Episode 81: Internal Medicine EOR Cardiology Questions appeared first on The Audio PANCE and PANRE.
68 ตอน
Podcast Episode 81: Internal Medicine EOR Cardiology Questions
The Audio PANCE and PANRE Physician Assistant Board Review Podcast
Manage episode 256904377 series 97199
เนื้อหาจัดทำโดย The Physician Assistant Life | Smarty PANCE เนื้อหาพอดแคสต์ทั้งหมด รวมถึงตอน กราฟิก และคำอธิบายพอดแคสต์ได้รับการอัปโหลดและจัดหาให้โดยตรงจาก The Physician Assistant Life | Smarty PANCE หรือพันธมิตรแพลตฟอร์มพอดแคสต์ของพวกเขา หากคุณเชื่อว่ามีบุคคลอื่นใช้งานที่มีลิขสิทธิ์ของคุณโดยไม่ได้รับอนุญาต คุณสามารถปฏิบัติตามขั้นตอนที่แสดงไว้ที่นี่ https://th.player.fm/legal
Welcome to episode 81 of the Audio PANCE and PANRE PA Board Review Podcast.
Join me as I cover ten internal medicine rotation EOR content blueprint questions from the Smarty PANCE physician assistant board and rotation review website.
Special from today’s episode:
- Check out the new Smarty PANCE Internal Medicine Rotation (EOR) Review Course
- Download your Free Trello Smarty PANCE PAEA Internal Medicine EOR Tracking Template
- Take the FREE Internal Medicine Rotation Cardiovascular Practice Exam
- View the interactive Smarty PANCE Internal Medicine Rotation (EOR) Topic List
Below you will find an interactive exam to complement the podcast.
The Audio PANCE/PANRE and EOR PA Board Review Podcast
I hope you enjoy this free audio component to the examination portion of this site. The full board review course includes over 2,000 interactive board review questions and is available to all members of the PANCE and PANRE Academy and Smarty PANCE.
- You can download and listen to past FREE episodes here, on iTunes, on Google Play Music or Stitcher Radio.
- You can listen to the latest episode, take an interactive quiz and download more resources below.
Listen Carefully Then Take The Practice Exam
If you can’t see the audio player click here to listen to the full episode.
Podcast Episode 81: Ten Internal Medicine EOR Cardiology Questions
The following questions are linked to PAEA Content Blueprint lessons from the Smarty PANCE and PANRE Board Review Website. If you are a member you will be able to log in and view this interactive video lesson.
1. 55-year-old woman is admitted to the hospital because she has shortness of breath and pain on both sides of her chest with deep breathing which has worsened over the past 5 days. In recent weeks, she has been feeling fatigued and has had low-grade fevers and night sweats, and was found to have a new cardiac murmur on examination. Her temperature is 38.1°C (100.6°F), pulse is 106/min, respirations are 26/min, and blood pressure is 136/88 mm Hg. She appears diaphoretic and is in mild respiratory distress. Cardiac auscultation reveals a faint systolic murmur heard over the lower left sternal border. Her neck veins are distended and abdominal examination shows hepatomegaly. Which of the following is the most likely cause of her clinical presentation?
A. Fat embolism
B. Infective endocarditis
C. Myocardial infarction
D. Rheumatic fever
E. Small cell lung cancer
Click here to see the answer
Answer: B, Infective endocarditis
Infective endocarditis (IE) is an infection of the endocardial surfaces of the heart, most commonly the heart valves. IE occurs when a microorganism begins to invade the heart valves causing an inflammatory reaction that damages the valve – sometimes leading to stenosis and sometimes leading to regurgitation. This patient developed a new cardiac murmur in recent weeks that is described as a faint systolic murmur heard over the lower left sternal border. This is most consistent with tricuspid regurgitation. She also has distended neck veins and hepatomegaly, both of which suggest right-sided heart failure which can result from tricuspid regurgitation. Small infectious emboli can break away from the primary lesion on the tricuspid valve and go into the pulmonary vasculature causing shortness of breath and pleuritic chest pain. Most cases of IE are caused by Staphylococcus aureus and Viridans streptococci, and diagnosis is confirmed by obtaining multiple blood cultures that show that there is continuous bacteremia.
- Fat embolism to the pulmonary circulation almost always occurs with major trauma, including surgical procedures like intramedullary nailing of long bones. Fat emboli can occlude the microvasculature, triggering a systemic inflammatory response. The woman did not have recent trauma, and a fat embolism would not explain her cardiac murmur.
- Clinical presentation of myocardial infarction most often includes substernal crushing chest pain, radiation of pain to the arms, left shoulder, back, neck, and jaw, as well as shortness of breath, anxiety, and fatigue. A myocardial infarction would not explain her developing a new cardiac murmur in recent weeks.
- Rheumatic fever is an autoimmune inflammatory process that develops as a sequela of streptococcal infection. Clinical manifestations include polyarthritis, carditis, erythema marginatum, chorea, and subcutaneous nodules. Rheumatic fever can cause some of the symptoms seen in this case, but the acute onset makes this option less likely.
- Although small cell lung cancer can present with pulmonary symptoms and low grade fevers, it wouldn’t easily explain her new cardiac murmur or the signs of right-sided heart failure.
Review PAEA EOR Blueprint Pearls With Links to Topic Lesson: Internal Medicine Rotation: Cardiovascular (PEARLS) ⇒ Endocarditis
2. A 54-year-old man comes to the emergency department following a four-day history of left-sided chest pain and shortness of breath. One week ago, he experienced upper respiratory symptoms along with myalgias and general fatigue. He has no known past medical history. He has not traveled outside the US. His temperature is 38.1°C (100.6°F), pulse is 104/min, respirations are 17/min, oxygen saturation is 94% on room air, and blood pressure is 100/72 mm Hg. Physical examination shows an ill-appearing man with bibasilar rales, jugular venous distention of 11 cm with no murmurs, rubs, or gallops, and 1+ bilateral pitting edema of the lower extremities. His labs are within normal limits and his blood cultures are negative. An echocardiogram shows an ejection fraction of 35%. Which of the following is the most likely cause of this patient’s condition?
A. Adenovirus
B. Coxsackie A virus
C. Staphylococcus aureus
D. Corynebacterium diphtheriae
Click here to see the answer
The answer is A. Adenovirus
Myocarditis in the United States is most commonly caused by a viral infection, typically adenovirus, coxsackie B, parvovirus B19, or others. It often presents with systemic symptoms such as fatigue and chest pain, but may cause sudden death.
- Though coxsackie B virus is one of the most common causal pathogens of acute myocarditis, Coxsackie A causes herpangina, aseptic meningitis, and hand, foot, and mouth disease.
- Staphylococcus aureus is a common cause of bacterial endocarditis, not myocarditis. Endocarditis is more likely to present with a new murmur and signs of distant emboli such as nail-bed hemorrhage and Janeway lesions.
- Corynebacterium diphtheriae is the causal agent of diphtheria, which may involve myocarditis. However, the patient would then most likely have other symptoms of the disease, including pseudomembranous pharyngitis, lymphadenopathy, or an arrhythmia.
Review PAEA EOR Blueprint Pearls With Links to Topic Lesson: Internal Medicine Rotation: Cardiovascular (PEARLS) ⇒ Myocarditis
3. A 42-year-old woman comes to the emergency department because of chest pain, dyspnea, and lightheadedness. She recently recovered from a presumed viral upper respiratory infection and has a 10-year history of systemic lupus erythematosus. Physical examination shows a decrease in systolic blood pressure by 20 mm Hg during inspiration. An ECG is shown here. Which of the following is the most likely diagnosis?
A. Aortic dissection
B. Tricuspid regurgitation
C. Pericardial effusion
D. Aortic stenosis
E. Mitral stenosis
Click here to see the answer
The answer is C. Pericardial effusion
Pericardial effusions are associated with a variety of causes, including autoimmune disorders and infectious pericarditis. If pericardial effusion leads to cardiac tamponade, patients may have pulsus paradoxus, or a decrease in systolic blood pressure during inspiration of more than 10 mm Hg. Certain ECG findings are characteristic for pericardial effusion. In particular, electrical alternans (shown by arrows) is highly specific for pericardial effusion (usually in association with cardiac tamponade) but not particularly sensitive. This pattern, characterized by beat-to-beat changes in the QRS axis in the limb and precordial leads, is caused by swinging of the heart within the accumulated pericardial fluid. Other common findings on ECG include sinus tachycardia and low QRS voltage.
- Patients with aortic dissection classically present with a tearing or ripping pain in the chest or back and may have a significant variation in systolic blood pressure between arms (not across respirations).
- The severity of tricuspid regurgitation varies widely, ranging from asymptomatic disease to symptoms of right-sided heart failure (hepatosplenomegaly, ascites, peripheral edema).
- Patients with aortic stenosis, the most common cause of left ventricular outflow obstruction, typically present with exertional dizziness or angina. In end-stage disease, symptoms may progress to heart failure.
- Mitral stenosis obstructs the flow of blood from the left atrium to the left ventricle and typically manifests as exertional dyspnea and decreased exercise tolerance.
Review PAEA EOR Blueprint Pearls With Links to Topic Lesson: Internal Medicine Rotation: Cardiovascular (PEARLS) ⇒ Pericarditis
4. A 57-year-old man comes to the emergency department because of intermittent, severe leg pain in both his calves for 2 weeks. He has a history of untreated high blood pressure, diabetes, and high cholesterol. For the past 3 years, the pain started after walking three blocks and only going away upon resting. In the past 2 weeks, he has had the same pain at rest. His temperature is 36.5°C (97.7°F), pulse is 78/min, respirations are 17/min, and blood pressure is 160/89 mm Hg. Examination shows both calves are atrophied and there is a paucity of hair, but no swelling or discoloration. Additionally, his lower calves are cool to the touch and dusky in appearance. Doppler ultrasound shows perfusion to both feet, and blood pressures of 35/20 mm Hg in the posterior tibial artery are obtained bilaterally. Which of the following is most appropriate next step in management?
A. Immediate high-dose statin therapy
B. Immediately consult vascular surgery
C. Intravenous alteplase
D. Pain control and discharge; refer to vascular surgery as an outpatient
E. Rest, elevate, and compress the affected leg
Click here to see the answer
The answer is B. Immediately consult vascular surgery
Peripheral vascular disease with intermittent claudication and signs of decreased perfusion should be examined using Doppler ultrasound and the ankle-brachial index (ABI). An ABI of <0.41 is grounds for the immediate surgical consultation.
- Statin therapy has shown to be effective in treating intermittent claudication. However, this intervention is appropriate only when the patient is deemed to be stable, and the risk of limb ischemia has been addressed.
- Alteplase (tPa) has been used to treat intermittent claudication, but its use is outside the scope of the emergency room. Treatments initiated in the emergency department are unfractionated heparin, aspirin, pain control, and positioning of the leg to maintain perfusion.
- The patient has significant impairment of perfusion to his legs. Discharge and vascular surgery follow-up as an outpatient would be inappropriate and likely to result in morbidity or mortality.
- While this leg should be rested, compression and elevation are the opposite of what is needed. These therapies will further decrease the blood flow to the leg and put the patient at increased risk of complications.
Review PAEA EOR Blueprint Pearls With Links to Topic Lesson: Internal Medicine Rotation: Cardiovascular (PEARLS) ⇒ Peripheral vascular disease
5. A 6-year-old boy comes to the pediatric clinic because of 4 weeks of fatigue and shortness of breath. His medical history is notable for poor follow-up with yearly check-ups, but his mother notes that he has been fairly healthy for the duration of his life, except for a “bad sore throat that needed antibiotics” about 6 months ago. On examination, the boy appears fatigued, but is appropriately oriented and responsive, and is generally non-toxic appearing. He is afebrile. Cardiac examination is notable for a widely split S2, a quiet S1, and point of maximum impulse displaced to the left. Which of the following is the next best step in the management of this patient?
Elimination tool
A. Digoxin
B. Long-term penicillin
C. Short-term course of clindamycin
D. Reassurance & routine care
E. Intramuscular ceftriaxone
Click here to see the answer
The answer is B. Long-term penicillin
Rheumatic heart disease is caused by autoimmune cross-reactivity following a Streptococcal infection. Development of antibody-mediated mitral valve damage is common. Long-term penicillin is suitable for acute treatment and prophylaxis from complications.
- Digoxin is a purified cardiac glycoside that is typically used in the treatment of various heart conditions, such as atrial fibrillation, atrial flutter, and heart failure that cannot be controlled by other medication. It is not recommended for use in rheumatic fever.
- Clindamycin is an antibiotic used to treat middle ear infections, bone or joint infections, pelvic inflammatory disease, strep throat, pneumonia, and endocarditis. Clindamycin is typically used as endocarditis prophylaxis for patients that are already receiving penicillin for secondary rheumatic fever prophylaxis.
- This patient is suffering from rheumatic fever, which can lead to rheumatic heart disease. This can cause significant carditis which manifests as congestive heart failure.
- Ceftriaxone is an antibiotic used to treat numerous bacterial infections, such as pneumonia, ear infections, skin infections, urinary tract infection, and meningitis. It is not used in the treatment of rheumatic fever.
Review PAEA EOR Blueprint Pearls With Links to Topic Lesson: Internal Medicine Rotation: Cardiovascular (PEARLS) ⇒ Rheumatic heart disease
6. A 35-year-old woman, gravida 2, para 1, comes to the office because of her first prenatal visit at 12 weeks’ gestation. She has no current concerns, and her first child was born without complications. She has a history of long-standing untreated hypertension. Her temperature is 36.5°C (97.7°F), pulse is 78/min, respirations are 17/min, and blood pressure is 150/89 mm Hg. Which of the following medications would most likely be appropriate as initial treatment?
A. Atenolol
B. Hydrochlorothiazide
C. Labetalol
D. Lisinopril
E. Losartan
Click here to see the answer
The answer is C. Labetalol
Chronic hypertension in pregnancy can be treated with some medications and labetalol is recommended as a first-line therapy for treatment of hypertension during pregnancy. Angiotensin-converting enzymes (ACE) inhibitors and angiotensin II receptor blockers (ARBs) should be avoided.
- Atenolol is a β-blocker medication, which decreases blood pressure by decreasing heart rate and stroke volume. It is contraindicated in pregnancy because it has been associated with fetal growth restriction. β-blockers considered safe in pregnancy are metoprolol and labetalol.
- Hydrochlorothiazide is a thiazide diuretic which decreases blood pressure via volume depletion. Diuretics do not cause fetal malformations but are generally avoided in pregnancy, as they prevent the physiologic volume expansion seen in normal pregnancy. They may be used in states of volume-dependent hypertension, such as renal or cardiac disease.
- Lisinopril is an angiotensin-converting enzyme (ACE) inhibitor which decreases blood pressure through inhibition of the renin-angiotensin-aldosterone system. ACE inhibitors and the closely related angiotensin-receptor blockers are contraindicated in pregnancy because of the risk of birth defects including renal dysgenesis and oligohydramnios.
- Losartan is an angiotensin II receptor blocker (ARB) which decreases blood pressure through inhibition of the renin-angiotensin-aldosterone system. ARBs and the closely related angiotensin converting enzyme (ACE) inhibitors are contraindicated in pregnancy because of the risk of birth defects including renal dysgenesis and oligohydramnios.
Review PAEA EOR Blueprint Pearls With Links to Topic Lesson: Internal Medicine Rotation: Cardiovascular (PEARLS) ⇒ Hypertension
7. A 42-year-old man comes to the office for a routine check-up. Medical history includes diabetes mellitus and a long history of smoking. Family history includes coronary artery disease. Temperature is 36.5°C (97.7°F), pulse is 78/min, respirations are 17/min, and blood pressure is 160/89 mm Hg. A repeat blood pressure taken 2 days later shows 143/88 mm Hg. Which of the following is most likely the best initial therapy?
A. Enalapril
B. Furosemide
C. Hydrochlorothiazide
D. Metoprolol
E. Nifedipine
Click here to see the answer
Answer: A. Enalapril
Hypertension in the setting of diabetes should be treated, with a goal systolic blood pressure of <130 mm Hg. The best first choice of medication is an angiotensin-converting enzyme inhibitor (ACEi).
Incorrect Answers:
- Furosemide is a loop diuretic that can be used to treat hypertension but it is not a first line agent. Unlike ACE inhibitors, loop diuretics have no renoprotective qualities and therefore are a worse initial choice in a hypertensive diabetic patient.
- Hydrochlorothiazide is a thiazide diuretic and a first-line agent for the treatment of hypertension in non-diabetic patients. It is relatively contraindicated in diabetes because it has the potential adverse effect of hyperglycemia. It may also precipitate attacks of gout by increasing uric acid concentrations.
- Metoprolol is a β-blocker that is used for the treatment of hypertension but is not a first line treatment. Also, β-blocker are contraindicated in asthma, as well as in diabetic patients due to its potential to mask signs of low blood sugar.
- Nifedipine is a calcium channel blocker that is used in the treatment of hypertension but it is not a first line therapy. It has no renoprotective effects, and commonly causes peripheral edema as an unwanted adverse effect.
Review PAEA EOR Blueprint Pearls With Links to Topic Lesson: Internal Medicine Rotation: Cardiovascular (PEARLS) ⇒ Hypertension
8. A 45-year-old obese Caucasian gentleman arrives at your clinic for a routine check-up after having some blood work done during a workplace health screening. He is found to have an LDL cholesterol level of 550 mg/dL. He states that his father and brother had high cholesterol and both died at a young age from a heart attack. He has a follow-up appointment with his cardiologist because of some occasional chest pain and abnormalities seen on his EKG. Additionally, you notice that he has well-demarcated yellow deposits around his eyes. He is started on high dose statin and his LDL at 12 weeks is 350 mg/dL. What is the next best step in this patient’s management?
A. Continue high dose statin, the patient’s LDL is at goal
B. Add niacin 100 mg three times daily
C. Add ezetimibe (Zetia) 10 mg daily
D. Add a PCSK9 inhibitor
E. Refer to a lipid specialist
Click here to see the answer
The answer is C: add ezetimibe 10 mg
If LDL-C is not at goal after 6-12 weeks the next best step for the treatment of familial hypercholesterolemia is to add ezetimibe 10 mg daily and check again in 6-12 weeks. If at that time the patient’s LDL is still not at goal (ideally < 150) refer to lipid specialist to consider adding a PCSK9 inhibitor.
Pearls
- Familial hypercholesterolemia (FH) is the most common autosomal dominant genetic disease. The clinical syndrome (phenotype) is characterized by extremely elevated levels of low-density lipoprotein cholesterol (LDL-C) and a propensity to early-onset atherosclerotic cardiovascular disease. In general, homozygotes manifest the disease at a much earlier age than heterozygotes and the disease is more severe.
- Homozygous FH patients are rare and have an estimated prevalence of approximately 1:300,000 to 1:400,000
- Heterozygous FH is estimated to occur in 1 in 200 to 250 individuals in the United States.
- It is estimated that about 7 percent of American adults have an untreated lipoprotein cholesterol ≥190 mg/dL but only 1.7 percent carry an FH mutation
- Patients with undiagnosed homozygous familial hypercholesterolemia (FH) develop severe, premature, atherosclerotic cardiovascular disease and die before age 20 in many cases.
- In patients with a negative or unknown family history, an untreated LDL-C level of ≥190 mg/dL (4.9 mmol/L) suggests FH. This value is greater than the 90th percentile for age and sex.
Diagnosis
- The diagnosis of heterozygous familial hypercholesterolemia (FH) is made with genetic testing or clinical criteria. A causative mutation in the LDLR, APOB, or PCSK9 gene(s) secures this diagnosis
- When genetic testing is not available or not felt to be necessary, you can use the Dutch Lipid Clinic Network criteria, which assigns points based on low-density lipoprotein cholesterol (LDL-C) levels, personal history of early atherosclerotic cardiovascular disease (ASCVD), family history of early ASCVD, or high cholesterol in a first-degree relative, and personal and physical examination finding
Treatment
- Patients with homozygous familial hypercholesterolemia (FH) – intensive LDL-C lowering, which targets a minimal value of <150 mg/dL (3.9 mmol/L)
- In addition to a high-dose statin (atorvastatin 80 mg daily or rosuvastatin 40 mg daily), most homozygous patients will require additional therapies such as ezetimibe, a PCSK9 inhibitor, or potentially LDL-C apheresis
Review PAEA EOR Blueprint Pearls With Links to Topic Lesson: Internal Medicine Rotation: Cardiovascular (PEARLS) ⇒ Hyperlipidemia
9. A 65-year-old man comes to the emergency department because of progressive dyspnea, coughing, and orthopnea. The patient says that over the past 2 months he has been feeling fatigued with ordinary physical activity. His medical history is relevant for dyslipidemia, type II diabetes mellitus, and a posterior myocardial infarction 4 months ago. Auscultatory findings reveal a pansystolic murmur over the mitral area. His temperature is 37.5°C (99.5°F), pulse is 90/min, respirations are 17/min, blood pressure is 120/90 mm Hg, and pulse oximetry on room air shows an oxygen saturation of 95%. This patient most likely has which of the following conditions?
A. Aortic stenosis
B. Aortic valve regurgitation
C. Mitral valve regurgitation
D. Mitral valve stenosis
E. Pulmonary stenosis
Click here to see the answer
The answer is C. Mitral valve regurgitation
Mitral valve regurgitation is defined as an incompetent closure of the mitral valve. Classically patients will present with a pansystolic heart murmur over the mitral area. Posterior myocardial infarction is the second most common cause of mitral valve regurgitation. Mitral valve regurgitation is characterized by an incompetent closure of the mitral valve. This condition causes retrograde blood flow into the left atrium during systole. The most common cause of mitral regurgitation is mitral valve prolapse, followed by a dysfunction of the posteromedial papillary muscle due to posterior myocardial infarction. Other causes may include, endocarditis or stretching of the mitral valve ring.
- Aortic stenosis is the reduction of the valvular orifice (<2 cm) with left ventricular outflow obstruction. Patients with aortic stenosis present with chest pain, syncopal episodes, and dyspnea. Here, the patient has progressive dyspnea (NYHA II), and a pansystolic murmur (mitral area), which relates to mitral valve regurgitation
- Aortic valve regurgitation (AOR) is described as an inefficient closure of the aortic valve leading to a retrograde blood flow into the left ventricle during diastole. Patients will present with a wide pulse pressure (Corrigan hammer pulse) or an Austin-Flint murmur (severe), none of which are present in this case.
- Mitral valve stenosis (MVS) is the reduction of the mitral valve orifice (<2.5cm). The left atrium becomes dilated and hypertrophied because of increased work of the left atrium. Patients with MVS present with dyspnea, rust-colored sputum, atrial fibrillation, and a diastolic heart murmur (diastolic rumble and opening snap).
- Pulmonary stenosis is an uncommon valvular lesion. It is commonly associated with congenital heart disease and carcinoid heart disease. Patients present a systolic ejection murmur in the left second intercostal space.
Review PAEA EOR Blueprint Pearls With Links to Topic Lesson: Internal Medicine Rotation: Cardiovascular (PEARLS) ⇒ Valvular heart disease
10. A 43-year-old man with a history of rheumatic fever comes to the primary care clinic for a check up. Cardiac examination reveals a late systolic crescendo murmur with midsystolic click best heard over the apex and loudest just before S2. Which of the following maneuvers will cause an earlier onset of the click/murmur?
A. Inspiration
B. Rapid squatting
C. Standing
D. Hand grip
E. Left lateral cubital position
Click here to see the answer
The answer is C. Standing
The ‘click’ of mitral valve prolapse, caused by the tightening of the chordae tendinae, moves closer to S2 with increased preload. Increased preload causes the left ventricle to stretch, as a result, the chordae tendinae are stretched as well. This makes it harder for the mitral valve to prolapse until the ventricles shrink enough to allow the chordae tendinae to let the mitral valve prolapse. Since there is more blood in the ventricles, it takes them longer to pump it out and shrink to a point at which MVP can occur, hence it occurs later in systole. Thus, the click will get closer to S2 with increased preload. Hand grip, rapid squatting, and inspiration all increase preload. Standing decreases preload and will cause an earlier onset of the click.
- The click of mitral valve prolapse is heard closer to S2 in the event of increased preload. Preload is increased by hand grip, squatting and inspiration.
- Placing the patient in the left lateral cubitus position will not affect preload and will have no effect on the timing of the click in mitral valve prolapse.
Review PAEA EOR Blueprint Pearls With Links to Topic Lesson: Internal Medicine Rotation: Cardiovascular (PEARLS) ⇒ Heart murmurs
Looking for all the podcast episodes?
This FREE podcast series is limited to every other episode, you can download and enjoy the complete audio series by becoming a Smarty PANCE member.
I will be releasing new episodes every few weeks. Smarty PANCE is now discounted, so sign up now before it’s too late!
Resources and Links From The Show
- Check out the new Smarty PANCE Internal Medicine Rotation (EOR) Review Course
- Download your Free Trello Smarty PANCE PAEA Internal Medicine EOR Tracking Template
- Take the FREE Internal Medicine Rotation Cardiovascular Practice Exam
- View the interactive Smarty PANCE Internal Medicine Rotation (EOR) Topic List
- Follow Smarty PANCE and The Daily PANCE Blueprint on Instagram
- Follow SMarty PANCE and The Daily PANCE Blueprint on Facebook
- My list of recommended PANCE and PANRE review books
- Interactive PANCE and PANRE NCCPA Exam Content Blueprints
- Sign up for the FREE Daily PANCE and PANRE email series
- Join the Smarty PANCE NCCPA Content Blueprint Website
- Get your free Trello PANCE study schedule
- Get 20% of any Picmonic membership by using this link
- Use Code “PALIFE” and get 10% OFF THE RUTGERS PANCE AND PANRE REVIEW COURSE
This Podcast is also available on iOS and Android
- iTunes: The Audio PANCE and PANRE Podcast iTunes
- Stitcher Radio: The Audio PANCE and PANRE Podcast Stitcher
- Google Play: The Audio PANCE and PANRE Podcast Google Play
![]()
Download The Content Blueprint Checklist
Follow this link to download your FREE copy of the PANCE Content Blueprint Checklist
Print it up and start crossing out the topics you understand, marking the ones you don’t, and making notes of key terms you should remember. The PDF version is interactive and linked directly to the individual lessons on Smarty PANCE.
Download for PANCE Download for PANRE
The post Podcast Episode 81: Internal Medicine EOR Cardiology Questions appeared first on The Audio PANCE and PANRE.
68 ตอน
ทุกตอน
×ขอต้อนรับสู่ Player FM!
Player FM กำลังหาเว็บ
ที่คล้ายกับ The Audio PANCE and PANRE Physician Assistant Board Review Podcast
The Art of Charm is where self-motivated people, just like you, come to learn from the company’s coaches about to how to master human dynamics, relationships, and becoming your best self with the help of Johnny and AJ, the company’s founders. Johnny and AJ bring their 11 years of coaching experience from their famous Bootcamps, where they host clients in Los Angeles from all over the world and they share their stories, best practices and themselves on this weekly podcast. Not only does The A ...
…
continue reading
A top podcast for healthcare leaders, with over one million downloads, Radio Advisory is your weekly download on how to untangle the industry's most pressing challenges to help leaders like you make the best business decisions for your organization. From unpacking major trends in care delivery—like site-of-care shifts and the rise of high-cost drugs—to demystifying stakeholder dynamics, to shining a spotlight on priorities that may get overlooked, we're here to help. Our hosts and seasoned r ...
…
continue reading
From the stuff your mother never told you, to the stuff your doctor never learned, On Health features taboo-busting conversations that demystify and de-stigmatize our bodies, all while bridging the gap between conventional medicine and wellness. Join Yale-trained MD & midwife Aviva Romm and her line-up of expert guests as they discuss everything from periods to menopause, sex to reproductive health politics, and motherhood to mental health. Each week, Dr. Romm will be exploring the science a ...
…
continue reading
How can business help solve society’s biggest challenges? Welcome to Series 3 of Take on Tomorrow, the award-winning podcast from PwC that examines the biggest problems facing society and the role business can—and should—play in solving them. This series, we’re welcoming broadcaster and journalist Femi Oke to the show. She joins podcaster and journalist Lizzie O’Leary, and together with industry innovators, tech trailblazers and visionary leaders from around the globe, they’ll explore timely ...
…
continue reading
From 4 x New York Times best-selling author Rachel Hollis comes the ultimate podcast for anyone looking for more joy and purpose in their lives. Featuring candid interviews with top performers in business, media, and lifestyle, as well as deep dives into topics like health and motivation, The Rachel Hollis Podcast has everything you need to level up your life!
…
continue reading
Join host and Harvard Business School Online Creative Director Chris Linnane as he sits down with HBS faculty to discuss business education in a way that’s both entertaining and insightful. The Parlor Room is your key to breaking down academic theory without sacrificing depth—all while gaining practical takeaways for navigating the business world.
…
continue reading
Join expert voices from Barbell Logic and others from the world of strength for resources to help you get strong for life. Get coaching options and more educational content at barbell-logic.com.
…
continue reading
Montgomery & Company (MoCo) is a weekly podcast and radio show hosted by two-time WNBA Champion and Co-Owner/Vice President of the Atlanta Dream, Renee Montgomery, in partnership with WABE Atlanta. Both insightful and compelling, MoCo features interviews with some of the world’s top athletes, entertainers, and innovators as well as roundtable discussions with Renee’s colleagues, friends, and family, about sports, culture and building generational wealth. Montgomery & Company: Sports, Cultu ...
…
continue reading
New episode every Wednesday! Join the Barbell Shrugged crew in conversations about fitness, training, and frequent interviews w/ CrossFit Games athletes!
…
continue reading
Welcome to Almost 30 - a supportive space to fuel your conscious evolution. Join us, LA-based best friends Krista Williams and Lindsey Simcik, for heart-centered, hilarious conversations and real, raw, impactful interviews with brilliant guests. We dive deep into topics like modern spirituality to health and wellness, aliens to entrepreneurship, social justice, and self development. With every episode, our mission is to empower you, expand what you think is possible and, make you laugh - a l ...
…
continue reading
Player FM - แอป Podcast
ออฟไลน์ด้วยแอป Player FM !
ออฟไลน์ด้วยแอป Player FM !




{kind=link}